Unisom
By J. Tuwas. United States Naval Academy.
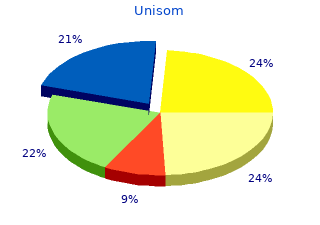
For instance buy 25 mg unisom mastercard, in a study reported by Ho and col- measure of IQ) purchase unisom 25mg amex, it was found that apparently healthy adoles- leagues (128), more than half of a sample of first-episode cents closer to their first hospitalization for psychosis per- patients with schizophrenia were found to be supported by formed more poorly than adolescents who were tested sev- public funds within 12months of their first episode of ill- eral years before their first exacerbation, but better than ness, and fewer than 25% of them had a job or went to patients whose disease had already exacerbated (125) (Fig. Furthermore, cognitive performance appears to be the part of some patients at the time of the first episode, slightly worse in patients with chronic disease (114) in com- continuing cognitive and functional deficit is the rule. In contrast to psychotic symptoms, including psychosis, are present many months to few years cognitive functions are less responsive to the neuroleptic before the formal diagnosis, and most, but not all, patients treatment administered for schizophrenia (126). Occupa- cognition with treatment, two separate studies demon- tional and cognitive deficits are clearly disproportionate strated modest longitudinal improvements in certain areas compared with the severity of psychotic symptoms in most of cognitive functioning (111,127). These findings suggest cases, despite evidence of improvement on the part of some diversity in the course of cognitive deficit even early in the patients. However, these results may be biased, because most illness, although they also indicate that there is no consistent first-episode studies enroll patients who (a) were sufficiently pattern of specific dimensions of improvement. Further- sick to need hospitalization, but (b) became sufficiently well more, even though an improvement in cognition was seen to be able and willing to consent to be followed-up after in these studies, no research to date has demonstrated that discharge, yet (c) are not sufficiently recovered to be com- many first-episode patients show evidence of normalization pletely out of the treatment network. More important, most in their cognitive functioning. Thus, although evidence of first-episode studies last less than 5 years because of attrition, worsening in cognitive functioning associated with duration funding, or other factors. Middle Course of Schizophrenia Until the early 1990s, the characteristics of schizophrenia in patients older than 55 years were largely the subject of speculation. As of 1993, it was estimated that less than 5% of all of the research ever performed on patients with schizo- phrenia had included any patients older than 55 years (129). It was 'common knowledge' that by age 55 to 60 years the illness has run its course, psychotic symptoms had burned out, and most patients did not need or did not benefit from medications. Since the early 1990s, however, Time until first admission a substantial amount of research on this topic has been completed, with this area one of the fastest developing as- FIGURE 47. Scores on the Ravens Progressive Matrices as a pects of research on schizophrenia. This research has consid- function of time until first admission for schizophrenia. One of the sources of the common knowledge that the Many of these questions are being addressed by a longitu- course of schizophrenia was established into old age was the dinal cohort study carried out by the Mt. Sinai School of consistent findings of symptomatic, cognitive, and func- Medicine group since the late 1980s, as well as other investi- tional stability on the part of patients after their first few gators who have become increasingly interested in this pop- episodes. Although many patients experience multiple psy- ulation. Most research on the course of func- in younger institutionalized patients (133). Many of these tional status suggests that the impairments noted at the time patients had cognitive and social performance compatible of the first episode are rarely reduced. Estimates of the pro- with dementia (136) that could not be accounted for by portion of patients with schizophrenia who are employed somatic treatment, lengthy institutionalization, poor moti- are in the range of about 40%, with most patients employed vation and education, or comorbidity. For example, in the in noncompetitive, sheltered settings (130). Likewise, inde- original publication on this population (133), it was demon- pendent living is the exception for patients with schizophre- strated that psychosurgery, insulin coma, electroconvulsive nia. There is also no significant evidence that functional therapy, and the severity of negative symptoms were not status in patients with schizophrenia changes markedly over the factors accounting for cognitive deficits. Relevant to the time or is altered by treatment with older antipsychotic issue of motivational deficits, in a subsample of the patients medications (131). This large body of data raises issues of from that study (137), the average level of education was importance when older patients are studied, including found to be more than 11 years, and their reading perfor- whether changes seen in later life are part of the natural mance was higher than the tenth grade level. In contrast course of the illness or whether they are the result of addi- to these indicators of educational achievement, the current tional comorbidities. Thus, some elderly institutionalized patients with schizophrenia appear Cognitive and Functional Deficits in to manifest decline in their functioning relative to premor- Older Patients bid functioning. It has been consistently reported, however, that many pa- Studies of the cognitive performance of elderly schizo- tients older than 65 years who have a lifelong course of phrenic patients have identified 'double dissociation' per- schizophrenia, especially those with a history of long-term formance profiles that discriminate them from patients with institutional care, have marked deficits in cognitive and clearly identified dementia (138–139), and a profile of dif- functional status (132–134). Similar findings have been re- ferential deficits has been identified. Differential deficits ported at different research sites in the United States and cannot be caused by a single constant factor, such as failing in the United Kingdom (135). Because of the lack of data to provide adequate effort when assessed. These data suggest regarding the lifetime course of functional and cognitive that studies of very poor-outcome long-stay patients, al- deficits in schizophrenia, it is not clear whether the presence though clearly reflecting the most seriously ill subset of the of severe deficits in functioning seen in these elderly institu- population, are not hugely biased by the obvious factors tionalized patients with schizophrenia is the result of deteri- associated with long institutional stay.
Insulin and insulin-like growth factor-1 comes long and stiff upon phosphorylation: correlation between regulate tau phosphorylation in cultured human neurons buy 25mg unisom overnight delivery. J Biol paracrystalline structure and degree of phosphorylation purchase unisom 25 mg on-line. Phosphorylation of Ser262 synthase kinase-3/factor A. A brain-specific activator of opment and contributes to reduced microtubule binding. Tau in paired helical filaments is function- to p25 deregulates Cdk5 activity and promotes neurodegenera- ally distinct from fetal tau: assembly incompetence of paired tion. Phosphorylation of Ser262 ylation of tau protein at Ser202/Thr205 in response to microtu- strongly reduces binding of tau to microtubules: distinction bule depolymerization in cultured human neurons involves pro- between PHF-like immunoreactivity and microtubule binding. Phosphorylation affects the ability of tau hyperphosphorylated forms of tau protein in human brain slices. Modulation of of protein phophatase 2A is associated with microtubules and the dynamic instability of tubulin assembly by the microtubule is regulated during the cell cycle. Vogelsberg-Ragaglia V, Schuck T, Trojanowski JQ, et al. Progressive su- proteins differentiate corticobasal degeneration and Pick disease. Different distribution caused by tau gene mutations. Vulnerable neuronal tion study of frontotemporal dementia in the Netherlands. Autosomal domi- in familial frontotemporal dementia (FTD-Kumamoto). Ann nant dementia with widespread neurofibrillary tangles. Pathogenic implica- exon 10 splice site region in familial frontotemporal dementia. Tau proteins with FTDP- families and kindreds with late-onset FAD. Neurology 1997;48: 17 mutations have a reduced ability to promote microtubule 949–954. Splice junctions, branch autosomal dominant parkinsonism and dementia with pallido- point sites, and exons: sequence statistics, identification, and ponto-nigral degeneration. The cardiac troponin T alternative parkinsonism-amyotrophy complex. Neurology 1994;44: exon contains a novel purine-rich positive splicing element. The role of exon sequences and parkinsonism linked to chromosome 17: a new group of tauopathies. A splicing enhancer of a chromosome 17-linked autosomal dominant parkinsonism in the human fibronectin alternate ED1exon interacts with SR and dementia ('pallido-ponto-nigral degeneration'). The regulation of splice-site selection, tau gene in familial multiple system tauopathy with presenile and its role in human disease. Polymerization tauopathy with presenile dementia is localized to chromosome of tau peptides into fibrillar structures. Accelerated filament disinhibition dementia: a frontotemporal dementia linked to formation from tau protein with specific FTDP-17 missense 17q21-22. Somatodendritic locali-¨ and 5′-splice-site mutations in tau with the inherited dementia zation and hyperphosphorylation of tau protein in transgenic FTDP-17. FTDP-17: an early- ing the shortest human tau isoform. Neuron 1999;24:751– onset phenotype with parkinsonism and epileptic seizures caused by a novel mutation. Prominent axon- dementia with a novel missense mutation in the tau gene. Neu- opathy in the brain and spinal cord of transgenic mice overex- roreport 1999;10:497–501. Axonopathy and amy-¨ Natl Acad Sci USA 1999;96:55598—55603. Tau gene mutation Acta Neuropathol (Berl) 2000;99:469–481. G389R causes a tauopathy with abundant pick body-like inclu- 179.
It has an insidious onset generic 25 mg unisom with mastercard, and patients often exhibit apathy unisom 25mg visa, cognitive and motor slow- although persons with HADmay experience an acceleration ing, and impaired memory, abstract reasoning, and judg- 1284 Neuropsychopharmacology: The Fifth Generation of Progress TABLE 90. DIAGNOSTIC CRITERIA FOR concentration, forgetfulness, mental slowing). In some pa- DEMENTIA DUE TO HIV DISEASE tients, HADprogresses rapidly after the diagnosis has been made (within weeks to months), whereas other patients A. The development of multiple cognitive deficits manifested by both show cognitive stability for months or years or very slow 1. Per- information or to recall previously learned information) and sons in the early stages of HADoften complain of poor 2. They typically present with significantly less impair- b. The cognitive deficits in criteria A1 and A2 each cause significant impairment in social or occupational functioning The later stage of HADcorresponds to ADC as originally and represent a significant decline from a previous level of functioning. Evidence from the history and physical examination or laboratory findings indicate that the disturbance is the direct TABLE 90. AIDS DEMENTIA COMPLEX STAGING physiologic consequence of HIV infection affecting the central SCHEME nervous system. Deficits do not occur exclusively during the course of a delirium. ADC Stage Characteristics Stage 0 (normal) Normal mental and motor function. HADrepresents the more severe end of a continuum characteristic of ADC, or mild signs of HIV-related cognitive deficits; the milder end is repre- (snout response, slowed extremity sented by the presence of a single cognitive impairment, movements), but without impairment of such as psychomotor slowing. The deficits observed in this work or capacity to perform ADL; gait disorder result in impaired social and occupational func- and strength are normal. Stage 1 (mild) Unequivocal evidence (symptoms, signs, tioning. Stage 2 (moderate) Cannot work or maintain the more Other causes, such as depression and delirium, which can demanding aspects of daily life, but manifest as cognitive impairment, must also be ruled out. Stage 3 (severe) Major intellectual incapacity (cannot be the direct pathophysiologic consequence of HIV disease follow news or personal events, and has outlined its own diagnostic criteria (Table 90. Price and Brew (66) argued that it is not enough simply Stage 4 (end stage) Nearly vegetative; intellectual and social to characterize HIV-infected persons as demented or not. J Infect Dis 1988;158:1079–1083, and Sidtis JJ, Gatsonis C, Price RW, et al. HADbegins with Zidovudine treatment of the AIDS dementia complex: results of a subtle deficits in cognitive processes (e. Chapter 90: Neuropsychiatric Manifestations of HIV-1 Infection and AIDS 1285 TABLE 90. CRITERIA FOR A CLINICAL DIAGNOSIS defined, and survival expectancy at this stage may be 6 OF HIV-1-ASSOCIATED COGNITIVE/MOTOR months or less. Features includes global cognitive dysfunc- COMPLEXa tion, significant functional impairment, and psychotic symptoms. Not sufficient for diagnosis of AIDS confusion, disorientation, delusions, hallucinations, sei- A. HIV-1-associated minor cognitive/motor disorder Probable (must have each of the following): zures, and muscular weakness and paralysis (particularly in 1. Cognitive/motor behavioral abnormalities (must have the lower limbs). Advanced dementia may result in disinhi- each of the following): bition, mutism, catatonia, and incontinence (5,60). At least two of the following acquired cognitive, ropsychiatric complications of late-stage HAD include motor, or behavioral symptoms (present for at least 1 depression, mania, and psychosis. Acquired cognitive/motor abnormality verified by An early prospective study of HIV infection in the United clinical neurologic examination or neuropsychological States revealed that HADdevelops in approximately 15% testing (e. The WHO cross-cultural study perceptual motor skills, attention/concentration, speed of processing of information, abstraction/ examining the neuropsychiatric consequences of HIV infec- reasoning, visuospatial skills, memory/learning, or tion represents the best study of the prevalence of HAD speech/ language) based on a diverse clinical sample. Disturbance from cognitive/motor/behavioral abnormal- persons at five sites around the world (Bangkok, Thailand; ities (see #1) causes mild impairment of work or activities Kinshasa, Zaire; Munich, Germany; Nairobi, Kenya; and of daily living (objectively verifiable or by report of a key informant). Does not meet criteria for HIV-1-associated dementia patients with AIDS ranged from 4. No evidence of another etiology, including active central Bangkok, no cases of HADwere recorded). In addition, no nervous system opportunistic infection or malignancy, or patients met the criteria for HADwhile in the asymptomatic severe systemic illness determined by appropriate history, physical examination, and laboratory and radiologic stage (11). In 1997, the CDC reported that 5% of adults investigation (e. The with an AIDS-defining opportunistic illness had HIV en- above features should not be attributable solely to the cephalopathy (dementia) (67).
The reasons for the underestimations differ from one of these disorders to the next discount unisom 25 mg. In the case of GAD discount 25 mg unisom amex, prevalence was underestimated in the early DIS surveys due to the fact PREVALENCES that the excessively unrealistic criterion in the DSM-III was operationalized by requiring that respondents endorse a Anew generation of psychiatric epidemiologic surveys, statement that they worried about things that were not really which began with the Epidemiologic Catchment Area serious or about things that were not likely to happen. This (ECA) Study in the early 1980s (9), has dramatically in- requirement is overly restrictive in two ways. First, there is creased our knowledge about the general population preva no requirement in DSM that people with GAD have insight lences and correlates of anxiety disorders. The ECAStudy into their worries being excessive or unrealistic. Although was the first psychiatric epidemiologic study to use a fully they must be aware that they worry more than other people structured research diagnostic interview designed specifi do, they can perceive others as worrying too little rather cally for use by lay interviewers to operationalize the criteria than themselves as worrying too much. Second, even in the of a wide range of mental disorders. This interview, known presence of a recognition that their worrying is excessive, as the Diagnostic Interview Schedule (DIS) (10), was used there is no requirement in DSM that the worries of people throughout the 1980s and early 1990s to carry out parallel with GAD must be exclusively focused on things that are epidemiologic surveys in a number of countries (11,12). Indeed, the heteroge The DIS was also used as the basis for an elaborated inter- neous worries that are characteristic of most people with view developed by the WHO and known as the Composite GAD (e. The CIDI children are going to turn out, neighborhood safety, global was designed to generate diagnoses according to the defini warming, etc. WHO auspices resulted that only about 3% of the population meet criteria for GAD in over a dozen large-scale, general-population CIDI surveys at any time in their lives (17). Early CIDI surveys followed being carried out around the world over the past decade. Subsequent CIDI surveys expanded the creation of the WHO International Consortium in Psy the assessment of excessive worry in GAD by asking re chiatric Epidemiology (ICPE) (14), which is currently coor spondents if there was ever a time in their lives when they dinating national CIDI surveys in 25 countries around the were worriers or when they worried a lot more than most world, with a combined sample size of over 150,000 re other people in their same situation, without requiring that Chapter 67: The Economic Burden of Anxiety and Stress Disorders 983 the worry be exclusively about things that are not serious Assessments of PTSD in epidemiologic surveys that used or not likely to happen. Prevalence estimates were found to the DIS led to the estimate that only about 1% of the be considerably higher when this modification was intro United States population meet criteria for this disorder at duced (20). Subsequent surveys that used In addition, these new studies investigated the implica the CIDI modified the assessment of PTSD by including tions of the requirements in the DSM-IV and ICD-10 that a detailed traumatic event checklist and by asking respon the worry in GAD persists for a minimum of 6 months and dents to give separate yes or no reports for whether each of found that this requirement might be too restrictive. In some CIDI surveys, particular, many people with chronic excessive worry report a visual checklist was used that aimed at making it easier having fairly short episodes, each of which lasts for several for respondents to report embarrassing events (e. Such individuals are currently ex 'Were you ever raped? CIDI PTSD symptom assessment cluded from a diagnosis of GAD and, because of their high proceeded very much along the same lines as the DIS after comorbidity with depression, are classified as being de- documenting that trauma exposure had occurred. Yet the pressed even though their most prominent symptoms are prevalence estimates obtained in the CIDI surveys were dra often associated with anxiety rather than depression. The matically higher than in the DIS surveys, with lifetime prev new WHO WMH2000 Initiative is investigating this mat alences as high as 12. This is assessed in a single question that presented respondents with important because epidemiologic surveys that include as a long checklist of feared situations and asked them if they sessments of current nonspecific psychological distress typi ever had unreasonably strong fears of these situations. In cally find that a high proportion of the respondents who addition to being mixed in with a number of specific fears, report clinically significant current distress in the anxiety- only five social phobic situations, all involving performance mood spectrum do not meet criteria for any of the anxiety fears, were included in the ECAlist. Given the extremely high prevalences of exposure the CIDI corrected this problem by screening for social to stressful events found in surveys of stress exposure (28), phobia with a separate, longer list of social fears (both inter it is plausible to think that many of these people have a actional and performance). These later surveys consistently diagnosis of either acute stress disorder or adjustment disor found social phobia to be much higher than in the DIS der. The new WHO WMH2000 surveys mentioned earlier surveys, with lifetime prevalences as high as 13% (18) and in this chapter are investigating this possibility by evaluating current prevalences as high as 8% (22). This seems to have been a criteria for other anxiety or mood disorders. Arough comparison is pro experience, such as combat in a war or sexual assault, and vided by the recently completed Midlife Development in that people who experience these events often have bad the U. Respondents were then asked if they ever lel assessments were made of commonly occurring physical had such an event that caused such reactions and, if so, to and mental disorders, along with assessments of the effects tell the interviewer what this event was. Subsequent de- of these disorders on day-to-day functioning (29). As in briefing showed that this question was too complex for most other health surveys of chronic physical conditions, many respondents, that the absence of a detailed event list of which a great many exist (e. However, past health surveys of 984 Neuropsychopharmacology: The Fifth Generation of Progress chronic physical conditions have seldom assessed emotional Increases for panic, specific phobia, agoraphobia, and obses disorders along with these physical disorders. In doing so, sive-compulsive disorder, in comparison, have been more the MIDUS survey found that 16. Although these studies have not investigated either ported an anxiety or stress disorder exclusive of either major acute stress disorder or adjustment disorder, separate evi or minor depression, and that an additional 14. These find consistent with the likelihood that the prevalences of these ings make anxiety-stress the fourth most commonly occur- disorders have also been on the rise (33).
These results were confirmed in a double-blind the GPi is similar to that for STN buy discount unisom 25 mg on line. As is the case with the crossover study (209) that led to the approval of unilateral STN purchase unisom 25mg online, the GPi is also overactive in PD (203,211), and le- DBS-VIM as a treatment for essential or parkinsonian sions of the GPi provide benefits in MPTP monkeys (219). Interestingly, stimulation slightly posterior prove all of the cardinal features of parkinsonism and reduce and medial to the VIM—close to the centromedian and the severity of levodopa motor complications (220–222). Unfortu- but a prospective controlled trial has yet to be performed nately, DBS-VIM does not meaningfully improve the more to objectively compare these two targets. This shortcoming has led to consideration of other targets for DBS, such as the GPi and the STN (see General Adverse Effects of DBS below). DBS-VIM remains a very valuable procedure for PD patients for whom tremor is the main handicap. Adverse effects of DBS can be related to the surgical proce- dure, the device, and the stimulation itself. Surgical compli- cations involve hemorrhage and infarction and occur in less Deep Brain Stimulation of the Subthalamic than 3% of cases. The electrode itself does not seem to be Nucleus (DBS-STN) toxic to local tissues, as in the only postmortem pathologic A large body of experimental evidence has pointed toward study available, gliosis around the electrode tip was less than targeting the STN as a treatment for PD: (a) neurons in 1 mm in diameter (223). Problems associated with the im- the STN are hyperactive in PD (203,211); (b) lesions of planted material (infection, dislodgment, mechanical dys- the STN provide benefit to MPTP-treated primates (204, function) occur in 1% to 3% of cases and may lead to the 205); (c) improvement in contralateral parkinsonism fol- need to replace the electrode. Stimulation-related side ef- lowing a spontaneous hemorrhage into the STN of a PD fects include paresthesiae, motor twitch, dysarthria, and eye patient (212); and (d) improvement in MPTP-treated mon- movement disorders. They are usually transient and control- keys following stimulation of the STN (213). Finally, the battery has lim- findings, DBS-STN was introduced as a treatment for PD ited longevity, ranging from 6 months to 5 years or more, patients (214–216). The battery in the chest wall can be easily (233–238). Results were somewhat inconsistent among the replaced under local anesthesia in most cases. In one study using a predeter- the risk of permanent side effects is less than with ablative mined transplant protocol, six PD patients who could not procedures, particularly when bilateral with procedures be improved with medical management experienced signifi- (224). The variability in Management of DBS clinical response in the different centers may have related Optimization of stimulator settings is necessary to achieve to the use of different transplant variables (e. This is not an easy method of tissue storage, target site for transplant, volume task because of the large number of stimulation variables. In trials documenting clinical ben- width, and frequency. Determination of the optimal stimu- efit, striatal fluorodopa uptake on PET demonstrated a sig- lation settings may be complicated and time consuming nificant and progressive increase in striatal fluorodopa (hours) and may require multiple visits. Benefits on PET correlated with im- rapid and simple method for determining stimulator adjust- provement in motor scores (238,241). Postmortem studies ment will enhance the utilization of these techniques. These studies demonstrated ro- this cannot otherwise be attained with medical therapy. Fur- bust survival of implanted neurons and reinnervation of the ther, this can be accomplished without the need to make a striatum in an organotypic fashion (242). In this study, destructive brain lesion with its accompanying side effects. Nevertheless, studies performed to Following these open studies, two prospective random- date indicate that this procedure has much to offer patients ized double-blind placebo-controlled trials have been initi- with advanced PD. STN appears to provide the best clinical effects and is pres- Two donors per side were implanted into the caudate and ently considered to be the stimulation target of choice. It putamen bilaterally, without immunosuppression (244). However, significant improvement in UPDRS superior in the future. The second study is a 2-year study that compares bilateral transplantation into the postcommissural putamen Transplantation Procedures with one versus four donors per side (174). Immunosup- Yet another approach to the treatment of patients with ad- pression with cyclosporine was employed in this study. The vanced PD is transplantation of dopaminergic neurons study is still ongoing and will terminate in 2001. Transplantation is a rational strategy plant procedures. In general, the procedure has been well for treating PD because (a) PD is due to specific degenera- tolerated, especially when performed in major university tion of dopaminergic nigrostriatal neurons and its symp- centers. There is one report of a death due to obstructive toms are dramatically relieved by dopaminergic treatment; hydrocephalus caused by graft migration into the 4th ventri- and (b) the striatum, which is denervated in PD, is a well- cle. Postmortem study revealed that the migrated tissue was defined target for transplantation (225).
Under conditions this portion of the nephron purchase 25mg unisom visa, but net potassium reabsorption is of potassium depletion 25 mg unisom with amex, the cortical collecting duct becom es a site closely coupled to sodium and water reabsorption. Decreases in total body potassium by electroneutral N a+-K+-2Cl- cotransport in the thick ascending increase pum p activity, resulting in enhanced potassium reabsorp- lim b, the low intracellular sodium and chloride concentrations pro- tion. This pum p m ay be partly responsible for the m aintenance of viding the driving force for transport. In addition, the positive m etabolic alkalosis in conditions of potassium depletion. The apical potassium channel allows potassium recycling and provides substrate to the apical N a+-K+-2Cl- cotransporter. Loop diuretics act by com - peting for the Cl- site on this carrier. Spurious hypokalem ia results when blood speci- m ens from leukem ia patients are allowed to stand at room tem perature; this results in leukocyte uptake of potassium from serum and artifactual hypokalem ia. Patients with spurious hypokalem ia do not have clinical m anifestations of hypo- kalem ia, as their in vivo serum potassium values are norm al. Theophylline poison- ing prevents cAM P breakdown (see Fig. Barium poisoning from the inges- tion of soluble barium salts results in severe hypokalem ia by blocking channels for exit of potassium from cells. Episodes of hypokalem ic periodic paralysis can be precipitated by rest after exercise, carbohydrate m eal, stress, or adm inistra- tion of insulin. H ypokalem ic periodic paralysis can be inherited as an autoso- m al-dom inant disease or acquired by FIGURE 3-7 patients with thyrotoxicosis, especially O verview of diagnostic approach to hypokalem ia: hypokalem ia without total body Chinese m ales. H ypokalem ia can result from transcellular shifts of potassium into anem ia is associated with potassium cells without total body potassium depletion or from decreases in total body potassium. In certain circumstances (eg, diuretics abuse), renal potassium losses may not be evident once the stimulus for renal potassium wasting is removed. In this circumstance, urinary potassium concentrations may be deceptively low despite renal potassium losses. Hypokalemia due to colonic villous adenoma or laxative abuse may be associ- ated with metabolic acidosis, alkalosis, or no acid-base disturbance. Stool has a rela- tively high potassium content, and fecal potassium losses could exceed 100 mEq per day with severe diarrhea. Habitual ingestion of clay (pica), encountered in some parts of the rural southeastern United States, can result in potassium depletion by binding potassium in the gut, much as a cation exchange resin does. Inadequate dietary intake of potassium, FIGURE 3-8 like that associated ith anorexia or a “tea Diagnostic approach to hypokalemia: hypokalemia with total body potassium depletion sec- and toast” diet, can lead to hypokalemia, ondary to extrarenal losses. In the absence of redistribution, measurement of urinary potassium owing to delayed renal conservation of is helpful in determining whether hypokalemia is due to renal or to extrarenal potassium loss- potassium; however, progressive potassium es. The normal kidney responds to several (3 to 5) days of potassium depletion with appropri- depletion does not occur unless intake is ate renal potassium conservation. In the absence of severe polyuria, a “spot” urinary potassium well below 15 mEq of potassium per day. Patients with acute m onocytic and m yelom onocytic leukem ias occasionally excrete large am ounts of lysozym e in their urine. Lysozym e appears to have a direct kaliuretic effect on the kidneys (by an undefined m echanism ). Penicillin in large doses acts as a poorly reabsorbable anion, resulting in obligate renal potassium wasting. M echanism s for renal potassium wasting associated with am inoglycosides and cisplatin are ill- defined. H ypokalem ia in type I renal tubular acidosis is due in part to secondary hyperaldosteronism , whereas type II renal tubular acidosis can result in a defect in potassium reabsorption in the proxim al nephrons. Carbonic anhydrase inhibitors result in an acquired form of renal tubular acidosis. The osm otic diure- sis associated with diabetic ketoacidosis FIGURE 3-9 results in potassium depletion, although Diagnostic approach to hypokalem ia: hypokalem ia due to renal losses with norm al acid- patients m ay initially present with a norm al base status or m etabolic acidosis. H ypokalem ia is occasionally observed during the diuret- serum potassium value, owing to altered ic recovery phase of acute tubular necrosis (ATN ) or after relief of acute obstructive transcellular potassium distribution. H ypokalem ia and m ag- nesium depletion can occur concurrently in a variety of clinical settings, including diuretic therapy, ketoacidosis, am inoglycoside therapy, and prolonged osm otic diuresis (as with poorly con- trolled diabetes m ellitus). H ypokalem ia is also a com m on finding in patients with congenital m agnesium -losing kidney disease. The patient depicted was treated with cisplatin 2 m onths before pre- sentation.
Neuropsychology is a specialized purchase unisom 25 mg overnight delivery, learned and skilled activity buy unisom 25mg free shipping. The heading, Psychological tests, is used to indicated a few available tests to the general student or clinician; these are not the stuff of “neuropsychological assessment”. Clock face The patient is given paper and a pencil/pen and asked to draw a clock face, including the numbers, and to set the hands at a particular time. This simple test has been used in neurology for many years (Battersby et al, 1956). Purpose – screening task for visuospatial and constructional difficulties. Scoring – A ten point scoring system has been developed. However, a scoring system is not usually needed in the clinical setting – people usually either pass or fail this test – of course, intelligence and education need to be considered, but most healthy people can do a pretty good job. Examples from the same individual at different times can be easily collected and compared. More than half a century since it was first described, the clock face tests has been used to reflect different progress in different dementia subtypes (Lee et al 2011). Draw a bicycle The patient is given paper and a pencil/pen and asked to draw a bicycle. It is a favourite of the current author, although it has received little attention in the clinical literature. The patient can then be asked to explain how the bicycle works (Lezak, 1976; pp330-331). This calls for mechanical reasoning, and can present a challenge. Trail making test There are two parts (A, B; Partington & Leiter, 1949). They test speed, attention, sequencing, mental flexibility, and of visual search and motor function. The task is for the patient to connect the numbers in order as quickly as possible. Part B includes numbers from 1 t o13 and letters from A to L sprinkled randomly on a page. The task is to connect the numbers and letters in order (1, A, 2, B, 3, C…) as quickly as possible. Various authorities provide norm sets (Davis, 1968). Distribution of Trail Making Scores (seconds) for Normal Population Age 20-39 40-49 50-59 60-69 70-79 Part A B A B A B A B A B 90%ile 21 45 22 49 25 55 29 64 38 70 75%ile 26 55 28 57 29 75 35 89 54 132 50%ile 32 69 34 78 38 98 48 119 80 196 25%ile 42 94 45 100 49 135 67 172 105 292 10%ile 50 129 59 151 67 177 104 282 168 450 Pridmore S. Rey complex figure This figure was first created/researched well over half a century ago (Rey, 1941). Methods of administration differ, some ask the patient only to copy the figure, and others ask the patient to create the figure from memory (various intervals). This test assesses visuospatial and constructional ability and visual memory. Interestingly, it was recently used to demonstrate that during major depression episodes the memory is impaired, but improves with remission (Hammer and Schmid, 2013). Scoring – many methods of scoring have been devised. For bedside testing the non-expert uses a pass/fail grading system and refers the patient for expert assessment if necessary. This test can be repeated (with due consideration to learning effect). The collected attempts over time provide a record of progress. Osterrieth (1944) was among the first to develop a scoring system. The components of the figure are identified according to the following list and then each component is assessed. Results can be listed as raw scores and percentiles. Five parallel lines with 2, crossing 3, lower right 13. Horizontal line within 13, continuing 4 to right 17. Square attached to 2, lower left For each of the 18 units Score Correct Placed properly 2 Placed poorly 1 Distorted of incomplete Placed properly 1 Placed poorly 1/2 Absent or unrecognizable 0 Maximum = 36 points Percentile Norms for Adults: Rey Complex Figure Trial Percentile 25 50 75 100 Copy 31 32 34 36 Memory 18 22 27 35 5. Controlled word association test (CWAT) The CWAT is mentioned in Chapter 27.