Cetirizine
By S. Kafa. University of Akron. 2019.
HIV-1 transmission cheap cetirizine 5mg fast delivery, by Services purchase 10mg cetirizine overnight delivery, National Institutes of Health, Health Resources and Services stage of infection. Diagnosis of HIV-1 infection in children younger than 18 mission per coital act, by stage of HIV-1 infection, in Rakai, Uganda. Working Group on Antiretroviral Terapy and Medical Management of 126. Guidelines for the use of antiretroviral agents HIV infection and the sexual transmission of HIV. Guidelines for prevention and treatment of opportunistic US Department of Health and Human Services, Centers for Disease infections in HIV-exposed and HIV-infected children. MMWR health policy and practice: the contribution of other sexually transmit- 2008;57:845–9. Guidelines for the use of antiretroviral agents in HIV-infected 1999;75:3–17. Guidelines for prevention and treatment of opportunistic infections 146. Chancroid: clinical manifestations, diagnosis and manage- in HIV-infected adults and adolescents. Trends in herpes simplex the management of persons infected with human immunodefciency virus type 1 and type 2 seroprevalence in the United States. JAMA virus: 2009 update by the HIV medicine Association of the Infectious 2006;296:964–73. Protocols for the confrmation of reactive rapid HIV tests. Recurrence rates in genital her- HIV in the United States: implications for HIV prevention programs. Ann Intern Med J Acquir Immune Defc Syndr 2005;39:446–53. Natural history of genital herpes cal settings are efective in reducing risk of HIV transmission among simplex virus type 1 infection. Incorporating HIV prevention into the medical care of persons 153. Polymerase chain reaction for living with HIV: recommendations of CDC, the Health Resources diagnosis of genital herpes in a genitourinary medicine clinic. Sex and Services Administration, the National Institutes of Health, and Transm Infect 2002;78:21–5. Once-daily valacyclovir to reduce the risk for detection of herpes simplex virus (HSV) DNA on mucosal sur- of transmission of genital herpes. Goldberg LH, Kaufman R, Kurtz TO, et al; Acyclovir Study Group. Long-term suppression of recurrent genital herpes with acyclovir: a 155. Fife KH, Crumpacker CS, Mertz GJ, et al; Acyclovir Study Group. Recurrence and resistance patterns of herpes simplex virus following 156. HSV type specifc serology in sexual cessation of ≥6 years of chronic suppression with acyclovir. J Infect Dis health clinics: use, benefts, and who gets tested. Use of a glycoprotein and valacyclovir for suppression of recurrent genital herpes and viral G-based type-specifc assay to detect antibodies to herpes simplex virus shedding. Genital herpes education and counseling: testing Sex Transm Dis 2001;28:99–104. Te psychosocial impact the acceptance of herpes simplex virus type 2 antibody testing among of serological diagnosis of asymptomatic herpes simplex virus type 2 adolescents and young adults. Te psychosocial impact of testing antibodies in subjects with culture-documented genital herpes simplex individuals with no history of genital herpes for herpes simplex virus virus-1 or -2 infection. Efect of herpes simplex genital herpes: a shorter 3-day treatment course compared with 5-day suppression on incidence of HIV among women in Tanzania. Efect of aciclovir on HIV-1 acquisi- for treatment of recurrent genital herpes simplex virus type 2 infection. Successful oral acyclovir blind, placebo-controlled trial. Frequent reactivation of herpes aciclovir in immunocompetent patients with recurrent genital herpes simplex virus among HIV-1-infected patients treated with highly active infections: a parallel-groups, randomized, double-blind clinical trial.
Age and sex effects for affect ties of frontal neocortex in obsessive-compulsive disorder cheap 5 mg cetirizine overnight delivery. Computerized volume mea- Arch Gen Psychiatry 1999;56:913–919 purchase cetirizine 10mg with mastercard. Ipsilateral subcortical on discrimination learning and performance. In: Delafresnaye atrophy associated with temporal lobectomy. Visual discrimination learning after selective volumetry. Developmental progression in human infants and and after cognitive behavioral therapy. Biol Psychiatry 2000;48: infant monkeys, and the neural bases of, inhibitory control of 294–300. New York: Academy of Science pletes serotonin from the developing cortex and alters thalamo- Press, 1990:267–317. Neuroimaging and neuropsychology of Basic Books, 1996. Perseverative interference in monkeys ison with rates in unipolar depression and normal controls. Arch following selective lesions of the inferior prefrontal convexity. An assessment of aphasia and related bolic rates in non-depressed patients with obsessive-compulsive disorders. Functional heterogeneity of the prefrontal cor- 138. Behav Neural Biol 1979;25: metabolic rates in obsessive-compulsive disorder. Br J Psychiatry 1994;164: J Neurophysiol 1989;61:331–349. Functional magnetic dorsolateral prefrontal cortex of the rhesus monkey. Exp Neurol resonance imaging of symptom provocation in obsessive-com- 1970;27:291–304. J Neuropathol Exp Neurol 1985;44: metabolism in anxiety disorders studied with positron emission 578–591. New York: Liss, 1986: regional cerebral perfusion abnormalities in obsessive-compul- 47–73. A small step for the cell, a giant leap for mankind: a 144. Elevated medial- hypothesis of neocortical expansion during evolution. Trends frontal cerebral blood flow in obsessive-compulsive patients: a Neurosci 1995;18:383–388. Regional develop- anatomy of CCK4-induced anxiety in normal healthy volun- ment of the brain in early life. Arch Neurol roanatomy of anxiety: a study of three disorders using positron Psychiatry 1937;38:725–743. Neuroanatomical to paroxetine treatment in obsessive-compulsive disorder. Systematic changes 1644 Neuropsychopharmacology: The Fifth Generation of Progress in cerebral glucose metabolic rate after successful behavior modi- 166. Changes in platelet fication treatment of obsessive-compulsive disorder. Arch Gen markers of obsessive-compulsive patients during a double-blind Psychiatry 1996;53:109–113. Serotonin uptake and imipra- tients treated with clomipramine. Arch Gen Psychiatry 1990;47: mine binding in the blood platelets of obsessive-compulsive 840–848. Peripheral markers in childhood-onset obsessive-compulsive disorder: revisualiza- of serotonin and dopamine function in obsessive-compulsive tion during pharmacotherapy. Regional mine binding and serotonin uptake in platelets of eight adoles- 133Xenon cerebral blood flow and cerebral 99mTc-HMPAO up- cent and ten adult obsessive-compulsive patients. J Am Acad Child Adolesc Psy- ture review of a compound prominent in 1H-NMR spectro- chiatry 1996;35:1647. Obsessive-compulsive epilepticus: 1H magnetic resonance spectroscopic imaging. Biol Psychiatry Cereb Blood Flow Metab 1994;14:373–382. Platelet 3H-imipra- spectroscopy in obsessive-compulsive disorder: evidence for neu- mine binding sites in obsessive-compulsive behavior. Biol Psy- ronal loss in the cingulate gyrus and the right striatum.
UBE3A purchase cetirizine 10 mg on line, for example cetirizine 5mg with visa, has an antisense tran- 4% (91–93), similar to the rate of fragile X in the general script that is expressed solely from the paternally derived MR population (94). This antisense transcript may play a role in the types of chromosomal abnormalities in autism, though not suppression of the nonexpressed allele, and mutations in necessarily disproportionately so. Likewise, there are subtle this transcript, therefore, could contribute to some cases of but significant differences between the behavioral pheno- AS (76). Thus, just as imprinting plays a pivotal role in types of the two disorders. Autism is characterized by social PWS and AS, it is likely to significantly influence the effect indifference and deficits in the perception of emotion, of 15q11-q13 abnormalities in autism as well. Duplications of large genomic segments are asso- by a trinucleotide repeat that expands as it is transmitted ciated with chromosomal abnormalities in a number of spe- to successive generations (96). Once this expanded region crosses a threshold AS duplication breakpoints (80). Another, located centro- (approximately 200 repeats), it becomes susceptible to meric to the PWS/AS critical region, is repeated an increased methylation, which inhibits transcription of FMR1. FMRP, and variable number of times in PWS/AS individuals (81). FMRP is expressed in numerous gion to recombination abnormalities or 'mistakes' (77), a tissues including fetal brain. Intracellularly, it is found in finding with support from data showing increased rates of the nucleus near the nucleolus and in cytoplasm in associa- Chapter 41: The Molecular and Cellular Genetics of Autism 557 tion with ribosomes. It may function, therefore, as a chaper- relatives of autistic probands, the presence of milder traits one molecule in the transportation of messenger RNA that are qualitatively similar to the defining features of au- (mRNA)from the nucleus to the cytoplasm (98). These collective traits, referred to as the 'broader au- function of this protein gives rise to FXS, however, remains tism phenotype' (BAP), were first observed by Kanner in unclear. These results are supported by several family studies tism (2). In accord with this, a sizable number of sex chro- using the family history method of assessment (105,106). In a reported that familial aggregation of the BAP was associated recent survey of a clinical population, six out of 265 (2. In the Iowa Autism Family Study autistic individuals referred for cytogenetic testing were (Piven and Palmer, submitted)familial aggregation of the found to have abnormalities of the sex chromosomes other BAP was higher in relatives from families with two autistic than fragile X (Wassink et al. In addition, two siblings (multiple-incidence families)than in families ascer- X-linked disorders, Turner syndrome and Rett syndrome, tained through a single autistic child. Relatives syndrome (45,X)females with maternally derived X chro- from multiple-incidence families, for example, were found mosomes had diminished verbal skills and social cognition to have (a)elevated rates of personality characteristics such compared to those with paternally derived Xs. Molecular as aloofness and rigidity, (b)diminished pragmatic language studies implicated a paternally imprinted disease locus that and speech abilities, (c)fewer quality friendships, and (d) escapes X-inactivation in distal Xp22. This paternal decreased scores on a number of specific cognitive measures imprinting could explain why karyotypically normal males (107–109). Two more affected individuals, thereby enabling extension of more XO autistic individuals have recently been reported, typically small autism pedigrees. Understanding the bound- one with a maternally derived X (102)and the other with aries and nature of the BAP may also help our efforts to an X of unknown origin (Wassink et al. Rett syndrome, considered to be a subtype of repetitive behaviors, or cognitive deficits)that may map on PDD, is a disorder occurring only in girls that is character- to separate genes that together cause the full syndrome of ized by mental retardation, loss of speech, and stereotypic autism. This approach to disaggregating complex pheno- hand movements after 1 to 2 years of normal development. Clearly, clarification of the genetically rele- expression (1). The evidence from sex chromosome abnormalities and from X-linked dis- RELATED DISORDERS orders with phenotypic similarities, however, suggests that such pessimism is premature, and that the X and Y chromo- Autism is characterized by dysfunction in three symptom somes should continue to be a focus of attention in autism. As autism is a heterogene- BROADER AUTISM PHENOTYPE ous, genetically complex disorder, it may be that each of these domains has unique, independent genetic determi- In addition to describing the hereditary basis of autism, nants. Studying disorders that resemble these individual do- family and twin studies have demonstrated, in nonautistic mains, therefore, may provide insight into their etiology in 558 Neuropsychopharmacology: The Fifth Generation of Progress autism. There are also related disorders, such as tuberous some Abnormalities). Additional research related to social sclerosis, and domains of investigation, such as immunoge- deficits that may have relevance to autism comes from stud- netics, that may provide insight into autism. For example, nematode worms that lack receptors for neuropeptide Y become strik- Disorders of Language ingly isolated in situations where they would normally con- gregate with other worms (118). Genetic variability in re- Specific language impairment (SLI)is a disorder character- ceptors for oxytocin/vasopressin in mice and other rodents ized by isolated impairment of language skills, and may is also associated with clear variability in social behavior be characterized by grammatical impairment, word finding (119).
For further explanation of the model buy cheap cetirizine 10mg line, (101 purchase cetirizine 10mg free shipping,117,161,263), and the habenula (e. Positive feedback loops, such as the one involving PPN and the STN (labeled 2) and the pathway through CM and the putamen (labeled 1) will tend to aggravate or enhance the abnormali- ties of discharge in the basal ganglia output nuclei associated with movement disorders, such as PD, whereas negative feedback circuits, such as a feedback involving CM and STN (not shown) will act to normalize neuronal discharge in the basal ganglia output nuclei. It is worth noting that via the CM nucleus, activity changes in the indirect pathway may influence the activity along the direct pathway. Thus, increased STN output in parkinsonism, by an action via GPi and CM, may result in a reduction of activity along the direct pathway. The pathophysiology of early parkinsonism may differ FIGURE 122. Model of the proposed rate changes in the basal from that of late parkinsonism in several aspect. For in- ganglia–thalamocortical circuitry under normal (left) and parkin- stance, increased STN output in early parkinsonism may sonian conditions (right). In parkinsonism, dopaminergic neurons in the the substantia nigra pars compacta (SNc) degenerate, have a compensatory function by increasing glutamatergic which results, via a cascade of changes in the other basal ganglia drive on SNc neurons. Thus, it has been shown that local nuclei, in increased basal ganglia output from GPi and SNr. This, injections of glutamate receptor blockers into the SNc sig- in turn, is thought to lead to inhibition of related thalamic and cortical neurons. In addition to the changes shown here, there nificantly worsen motor signs in early stages of MPTP- are prominent alterations in discharge patterns (see text). MPTP-treated primates reverse all of the cardinal signs of At the same time, increased glutamatergic drive onto surviv- parkinsonism, presumably by reducing GPi activity (16,30, ing SNc neurons may also be (excito-) toxic (239). Similarly, GPi and SNr inactivation have been shown The reciprocal changes in activity in the indirect and to be effective against at least some parkinsonian signs in direct pathways following dopamine depletion should both MPTP-treated primates (179,181,308,315). The 2-deoxyglucose proaches to the treatment of medically intractable PD. This studies mentioned above demonstrated increased (synaptic) was first employed in the form of GPi lesions (pallidotomy) activity in the VA and VL nucleus of thalamus (60,201, (19,85,169,183,276,301) and, more recently, with STN le- 252), presumably reflecting increased inhibitory basal gan- sions (108). In addition, high-frequency deep brain stimula- glia output to these nuclei. Consistent with this are positron tion (DBS) of both the STN and GPi have been shown to emission tomography (PET) studies in parkinsonian pa- reverse parkinsonian signs. The mechanism of action of tients that have consistently shown reduced activation of DBS remains controversial. It appears most likely, however, motor and premotor areas in such patients (42,48,54,88, that DBS and lesions act similarly in that both result in an 90), although no changes have been seen in the thalamus. Alterations of cortical activity in motor cortex and supple- PET studies in pallidotomy patients performing a motor mentary motor areas have also been demonstrated with sin- task have shown that frontal motor areas whose metabolic gle-cell recording in hemiparkinsonian primates (306). For instance, the movement-related output from the parkinsonian signs. DBS of the STN and GPi have revealed SNr appears to reach predominately premotor areas, and similar changes with PET, further supporting this concept could conceivably play a role in some aspects of akinesia as well as the belief that DBS appears to act functionally (141). In addition, the SNr carries a substantial portion of like ablation. Abnormal SNr The experience with inactivation or deep brain stimula- discharge may therefore be associated with some of the non- tion of the SNr is very limited at this point. There are no (limb)-motor abnormalities in parkinsonism, including oc- studies of the effects of (exclusive) lesioning of the SNr ulomotor disturbances as well as cognitive, behavioral, and available, and one case report on the effects of (inadvertent) emotional disturbances. This clearly needs further study, but it that lesions of this nucleus in normal monkeys can lead seems that the SNr may not be a feasible target for surgical to hemiakinesia, possibly by reducing stimulation of SNc interventions, because of its prominent involvement in non- neurons by input from the PPN, or by a direct influence on motor functions, and possibly also because of the greater descending pathways (51,146,162,206). It remains unclear, degree of overlap between the different functional territories however, whether the motor abnormalities seen after PPN in this nucleus (123,127,186). It is noteworthy that these animals do not manifest rigidity or tremor, which appear It has long been clear that the aforementioned models of to be critically dependent on thalamic circuitry (see below). Changes that arise in any portion of the complex mental features of the disease. Thus, although the results basal ganglia–thalamocortical circuitry will have significant of lesions in parkinsonism seem at first glance easily ex- consequences in all other areas of the network. This implies plained by the above-mentioned rate-based model of par- that the search for a parkinsonism-inducing 'source' of kinsonism, more detailed studies of the results of lesions in abnormalities in the neuronal activity within the network patients with parkinsonism have brought to light several may be futile, but suggests also that surgical or pharmaco- important findings that are not compatible with the models. This can indeed be appreciated when based models, lesions of the 'basal ganglia–receiving' areas considering the results of lesion studies in parkinsonian pri- of the thalamus (VA/VL) do not lead to parkinsonism and mates. One of the most important and dramatic in this in fact are beneficial in the treatment of both tremor and 1768 Neuropsychopharmacology: The Fifth Generation of Progress rigidity (45,109,220,290)). Similarly, lesions of GPi in the lesions suggest that in patients with PD and other move- setting of parkinsonism lead to improvement in all aspects ment disorders the absence of basal ganglia input to the still of PD without any obvious detrimental effects. Further- intact portions of the basal ganglia–thalamocortical net- more, they are, often in the same patient, effective against work is more tolerable than abnormal input. Near-normal both parkinsonism and drug-induced dyskinesias (217, motor function is still possible in these disorders once the 235). In contrast to the abnormalities seen in parkinsonism, abnormal basal ganglia–thalamocortical input is removed.
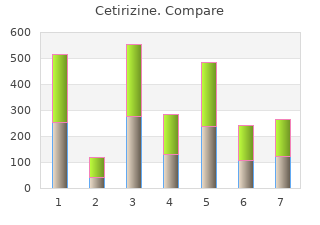
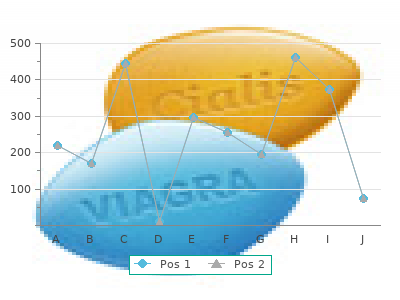
M ost transplant centers screen potential candi- coworkers generic cetirizine 10 mg with visa. H ypercholesterolem ia and hyper- triglyceridem ia are com m on after kidney 45 30 transplantation purchase cetirizine 10mg on line. Approxim ately two thirds of transplant recipients have low density 30 20 lipoprotein (LDL) or total cholesterol levels 74% 63% signifying increased cardiac risk; 29% have 15 10 elevated triglyceride levels 2 years after 0 0 transplantation (Kasiske, Unpublished 100 200 300 400 70 130 190 250 310 data). N ot only is hyperlipidem ia a clear risk factor for coronary disease (see Figs. Cholesterol, mg/dL LDL, mg/dL 13-13 and 13-14), but it may also contribute 75 40 to the progressive graft dysfunction associated n=588 n=430 with chronic rejection [21,22]. In The indications for lipid-lowering therapy and its goals are based addition to elevated low density lipoprotein (LDL) cholesterol levels, on the clinical history, risk factor profile (see Fig. About 40% of recipients are CHD— coronary heat disease. Sm oking, hypertension, and hyperlipidem ia are am ong the risk factors m ost am enable to long-term m odification. Although dose reduction can reduce lipid levels, it m ay also CyA increase the risk of acute rejection. As depicted, early experience in a large m ulticenter p<0. FIGURE 13-17 FIGURE 13-16 In the current era of im m unosuppressive therapy, hypertension A recent m eta-analysis of published trials in renal transplant affects roughly two thirds of transplant recipients. Unlike hyperten- recipients dem onstrated these benefits of the various treatm ents. These m ay be grouped dysfunction or rhabdom yolysis. These adverse events m ay occur conveniently into those originating within the allograft (intrinsic) m ore frequently in transplant recipients owing to the effect of and those originating elsewhere (extrinsic). Levels of 3-hydroxy-3-methylglutaryl coenzyme A (HM G CoA) reductase inhibitors are substantially higher in patients receiving both drugs. HDL— high density lipoprotein; LDL— low density lipoprotein. In these patients it m ay be possible to approach diagnosis and therapy in a fairly Blood pressure ≥140/90 standardized fashion. In transplant recipients with blood pressure readings consistently over 140/90 mm Hg, intervention is warranted. Evaluate allograft function The initial approach includes assessm ent of allograft function, Yes No extracellular fluid volum e (ECF) status, and im m unosuppressive dosing. If these variables are stable, it is reasonable to proceed with Optimal blood levels Reduce dose of antihypertensive therapy. Calcium antagonists (CA) are effective of cyclosporine cyclosporine or or tacrolimus? No tacrolimus agents and m ay offer the added benefit of attenuating cyclosporine- Yes induced changes in renal hem odynam ics. Verapam il, diltiazem , nicardipine, and m ibefradil increase blood levels of cyclosporine ECF volume status Consider salt restriction and tacrolimus and should be used with caution. No and/or diuretic with CAs that m ay lim it their use include cost, refractory edem a, Yes and gingival hyperplasia. Angiotensin antagonists (ACEIs and Administer receptor antagonists) are also effective; their use requires close Intervention fails to antihypertensive agent monitoring of renal function, serum potassium levels, and hematocrit normalize BP (CA, ACEI, or other) levels. Diuretics frequently are useful adjuncts to therapy in recipients owing to the salt retention that often accom panies cyclosporine M ultidrug regimen: Adequate response add agents of different use. O ther antihypertensive m edications offer no particular benefits to therapy? No classes as necessary or drawbacks and can be em ployed as needed. The rationale of Yes m ultidrug therapy is to em ploy agents that block hypertensive responses via interruption of differing pathogenetic pathways. As antihypertensive drugs are added, this consideration should Yes rem ain param ount [31,32]. GFR— glom erular filtration rate; Yes No TRAS— transplanted renal artery stenosis. Continue Re-evaluate allograft antihypertensive therapy function and drug therapy Reassess periodically Consider TRAS FIGURE 13-19 Transplant renal artery stenosis (TRAS). TRAS accounts for less than 5% of cases of hypertension after transplantation.
A polymorphism of the Catchol-O-methyltransferase (COMT) gene may contribute to personality disorders order cetirizine 5mg without prescription, especially where anxiety is a feature (Montag et al generic cetirizine 10mg on-line, 2012). Epigenetics Epigenetics is promising to provide unprecedented insight into the biology of personality disorder. Epigenetics refers to environmental events causing the attachment to, or removal from, DNA (not altering the DNA sequence), molecules (such as methyl groups) which influence gene expression. This is the molecular mechanism by which environmental influence on DNA produces the phenotype. Examples of epigenetics extending our understanding of personality disorder: 1. People who are sexually abused as children have altered methylation of hippocampal GR gene (McGowan et al, 2009). When people with borderline personality disorder are effectively treated with psychotherapy, there is a modification of the methylation of the brain derived neurotropic factor (BDNF) gene (Perroud et al, 2013). Child sex abuse leads to a) methylation of the promoter region of the serotonin gene, and b) female antisocial personality disorder – it is probable that methylation is the mechanism which links the abuse and the disorder (Beach et al, 2011; Nemeroff, 2016). Correlations have been demonstrated (Martin-Blanco et al, 2014) between childhood maltreatment and GR gene methylation, and between the extent of GR methylation and clinical severity of borderline personality. Immune system Disrupted immune activity has been advanced as a feature of many psychiatric disorders (see Chapter 34: Psychoneuroimmunology). Aetiology In common with other psychiatric disorders, the aetiology of personality disorders appears to be multifactorial, involving genetic, prenatal, early life experience, epigenetic and precipitating and perpetuating factors. Prenatal factors including hormone and alcohol exposure, intrauterine nutrition, and birth complications such as hypoxia, can all impact on personality. Temperament refers to aspects of personality which are considered innate, rather than learned, and can be observed in babies from birth. A mismatch between the temperament of the child and the temperament of the parents makes for a difficult relationship, and this may predispose to the development of behavioural and personality disorders. By definition personality disorders are long lasting. Contributing factors may include unhealthy early life experiences. However, personality disorder may only become apparent with the loss of an important support, such as caring parent, or when the individual is exposed to additional stress, such the responsibility for the care of a new baby. Features of personality disorder may perpetuate the disorder – for example, illegal drug use, aggressive outbursts, and inappropriate sexual provocation damage relationships and lead to additional losses, distress and anger. The individual with a personality disorder has limited ability to deal with stress in an adaptive manner, thus, limited ability to halt self-reinforcing, maladaptive cycles. Prognosis Prognosis depends on the nature and severity of the personality disorder. Cluster B disorders, characterized by erratic and impulsive behaviour usually improve with age (after 35 years). These people (as with the rest of us) mature over time and become less volatile, violent and irritable. Cluster C disorders, characterized by anxious and fearful disposition tend to become more confident and assertive. Cluster A disorders, characterized by eccentricity, may not change markedly. Borderline personality disorder is often thought of as a chronic, unremitting disorder. Pessimism regarding the prognosis in Cluster B disorder may be because a small number of people with severe borderline personality disorder can overwhelm regional resources. While remission of this disorder may occur, impaired social functioning commonly remains, and only about one third find employment. Management Management begins with a full assessment and the exclusion of other psychiatric disorders, such as major depression. Comorbid conditions should be managed in the standard manner. Treatment depends on the nature of the personality disorder, patient willingness to engage in treatment and the available resources (availability of specialist psychotherapists and treatment programs). Prolonged treatment may be necessary and complete recovery is the exception rather than the rule. Individuals with antisocial personality disorder are usually unable to co- operate and maintain a therapeutic relationship and are generally regarded as untreatable in all but specialized (usually forensic) units. Both dynamic psychotherapy (with roots in Freudian analysis) and cognitive behaviour therapy (which is focused more on thinking processes and behaviour) have much to offer.
Patients have sin (19) 10 mg cetirizine fast delivery, or prolactin (20) order cetirizine 10mg otc, and clinical response to ECT difficulty understanding how a treatment that is so seem was not shown in studies of depressed patients receiving a ingly toxic to the brain (i. ECT have focused less on the quantitative analysis of seizure However, the antidepressant medications have a number of duration and more on the relationship between a qualitative other effects on a variety of neurotransmitters, regulatory analysis of the ictal and postictal seizure morphology to hormones, and cellular mechanisms. ECT-induced seizures have a The mechanism by which a convulsive stimulus acts as characteristic pattern of hypersynchronous neuronal dis one of the most powerful antidepressants is equally complex charge with excitation of cortical neurons during the initial but the explanation may be as simplistic: ECT works by tonic phase, followed by alternating excitatory and inhibi increasing natural brain substances that decrease the excita tory effects in the clonic phase, and finally postictal suppres bility of the brain. The unique therapeutic action of ECT sion owing to inhibition and neuronal hypoexcitability. Seizure termination is an tered, and the stimulus waveform (23). A number of features active process that underlies the therapeutic mechanism of of the ictal EEG seizure that demonstrate a more intense the treatment. This idea is elaborated on in the following seizure predict clinical response to ECT. The initial finding was that an ECT seizure had to characteristics have been used to predict the efficacy of an continue for at least 25 seconds to be therapeutic (13) and ECT course (22,25–27), or more precisely these variables the patient had to accumulate a minimal number of seconds can be used to predict when a seizure is not adequate. Inade of EEG seizure time during a course of ECT (14). Chapter 76: Electroconvulsive Therapy 1099 Analysis of the EEG morphology has been used to deter- 1 minute and there is an active inhibitory process in the mine seizure intensity (26). Clinicians can be trained to interictal and postictal states evident by the development of visually inspect the EEG strips during ECT and determine slow or delta waves and decreases in the CBF and metabolic the adequacy of the seizure by evaluating the amplitude of uptake of glucose. The anticonvulsant properties of ECT the ictal EEG relative to baseline, symmetry of right and are hypothesized to occur because of enhanced transmission left hemispheric EEGs, distinct spike and wave pattern, and of inhibitory neurotransmitters and neuropeptides (e. Both the Thymatron GABA and endogenous opioid concentrations) and are an DGx ECT device (Somatics Inc. The magnitude of the seizure threshold increase is greater Although further testing of the clinical use of the computer- in more effective methods of administering ECT (i. Clinically, Sackeim in patients administered UL ECT, in determining if a sei cites unpublished data that the patients who return to an zure is adequate (24,27,29). However, nism of ECT is research correlating functional brain imag it is unclear whether the return of the seizure threshold to ing with response to ECT. Studies have shown an increase baseline occurs after an acute course of ECT in all patients in cerebral blood flow (CBF) up to 300% of baseline values or only in patients who relapse. The duration of the seizure with an accompanying increased permeability of the is also decreased over a series of treatments and is another blood–brain barrier and increased cerebral metabolic rate indication of the anticonvulsant effect of ECT. However, (CMR) up to 200% during the ictal period (30). In contrast, seizure duration is not related to efficacy unlike seizure CBF decreased to levels below baseline (31) or returned to threshold (43). Inhibitory processes include the early onset with clinical response, Nobler and colleagues (34) found a of high amplitude slow-wave activity after the tonic phase correlation between decreased CBF in the immediate postic of the seizure and bioelectric postictal suppression processes tal period and clinical response. The efficacy of ECT has been correlated included 54 depressed patients imaged using the Xenon with the early onset of these inhibitory processes, a fact that inhalation technique. Patients showed a low baseline CBF supports the anticonvulsant hypothesis. Two elements of compared to matched controls, and their response to ECT seizure expression, seizure strength and peak amplitude of was correlated with the further decrease in CBF from base- slow-wave activity, were inversely correlated with seizure line. These changes were greatest in the anterior cortical threshold and the third element, postictal bioelectric regions and the degree of change was correlated with clinical suppression, was not related to seizure threshold (40). Be- improvement on the Hamilton Depression Rating Scale. This finding provides the rationale Nobler and Sackeim (35) point out that decreased CBF in for developing EEG algorithms (see the preceding), increas the anterior cortex supports earlier findings by Max Fink ing the stimulus dosing or retitrating the seizure threshold (36,37) and their own group (38) of a relationship between during a course of ECT in patients who are not responding. There During a course of ECT, as in epilepsy, CBF/ CMR are additional data suggesting that the reductions in cerebral increase dramatically during the seizure and decrease below blood flow that occur immediately after ECT may persist baseline in the interictal and postictal states (35). Patients for days (39) to months (40) after the treatments and the responding to ECT show a more marked global decrease most dramatic reductions occurred in the frontal cortex. These changes were correlated with an increase findings with preclinical research in the anticonvulsant hy in the seizure threshold. Finally, increasing slow-wave activ pothesis as the mechanism of action of ECT (40). Both these finding and seizure duration decreases during the first several treat support the anticonvulsant hypothesis. ECT seizures usually are limited to less than The anticonvulsant hypothesis unifies many research 1100 Neuropsychopharmacology: The Fifth Generation of Progress findings and provides important new leads that have the reason for this apparent decline in efficacy is the increasing potential for improving clinical outcomes and predicting resistance to treatment among the patients referred for ECT patients who are at risk of relapsing after ECT. Prior to the development of the seroto vulsant properties of ECT related to clinical outcome in nin reuptake inhibitors (SSRIs), the most common reason clude an increase in the seizure threshold during a course of for referral for ECT was intolerance of available antidepres ECT, early onset of slow-wave activity interictally, distinct sant medications, chiefly tricyclic antidepressants (TCAs), postictal suppression, and decreases in CBF/CMR and in- and monoamine oxidase inhibitors (MAOIs). Intolerance creased slow-wave activity after a series of treatments. The elderly are also the patient group are rarely associated with seizures) and anticonvulsant medi most susceptible to the side effects of TCAs and MAOIs. However, there take inhibitors (SNRIs), 5-HT2A blockers, and other novel is evidence that newer anticonvulsant medications, includ antidepressants in the last 15 years has radically changed ing lamotrigine, may be more effective in the depressed the medication histories of the patients referred for ECT.